


Introduction
While classical psychedelics such as psilocybin and LSD show significant therapeutic promise for refractory mental health conditions, their rising prevalence in uncontrolled environments increases the risk of “bad trips” characterized by severe paranoia or anxiety. Most such episodes self-resolve within 24 hours, yet extreme cases may reach a level of severity that requires clinical intervention to restore psychological stability. This review addresses a critical gap in the literature by identifying the most effective pharmacological agents to manage acute distress when standard non-pharmacological containment strategies fail to provide adequate stabilization.
Infographic
Audio Summary
Key Findings
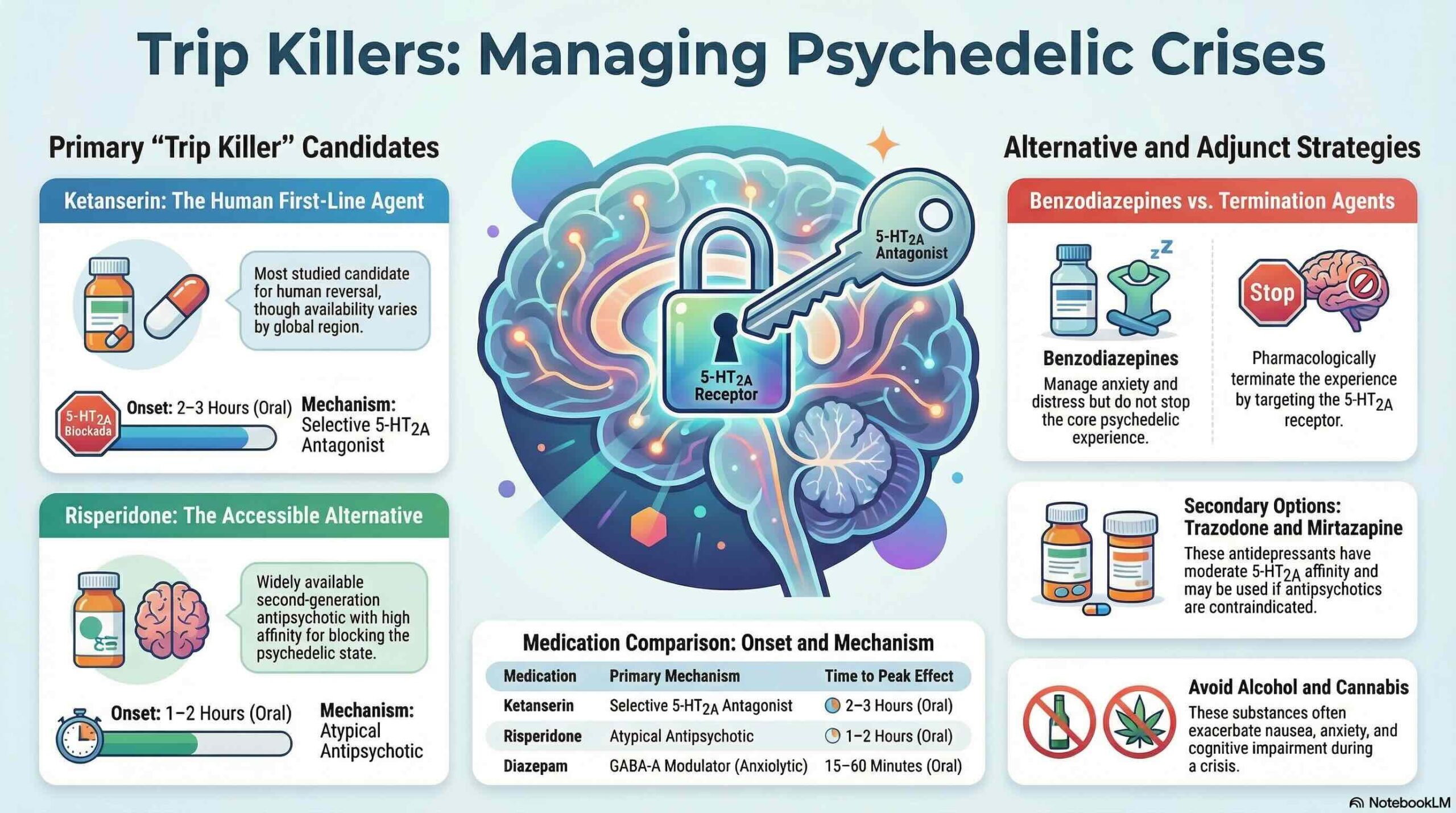
The primary biological mechanism for terminating a psychedelic experience is the functional antagonism of the 5-HT2A receptor. Ketanserin is currently the most evidence-supported agent for reversing the effects of LSD and psilocybin in humans, though its clinical utility is limited by low availability in US and UK markets. From a psychopharmacological perspective, the effectiveness of an antagonist is dictated by its binding affinity (Ki) and its residence time at the receptor. This is particularly crucial for LSD, where an “extracellular lid” folds over the binding pocket to trap the agonist; consequently, rapid-acting antagonists with high binding affinity are required to displace the drug and achieve functional termination of the state.
Due to their widespread availability, atypical antipsychotics serve as the leading practical alternatives for clinicians. Risperidone is a primary candidate due to its high 5-HT2A affinity and potent functional profile; notably, the review cites data indicating that 1 mg of risperidone can block 98% of psilocybin’s effects. In contrast, first-generation antipsychotics like Haloperidol should be avoided in these contexts, as they lack significant 5-HT2A activity and may be detrimental, potentially exacerbating anxiety without reducing hallucinatory symptoms. Other candidates include Trazodone, which possesses moderate 5-HT2A affinity, while benzodiazepines provide symptomatic relief through anxiolysis and sedation rather than directly terminating the core psychedelic state.
Despite the efficacy of pharmacological interventions, the authors emphasize that non-pharmacological strategies should remain the clinical priority. Psychological containment (emotional space-holding) and low-stimulus environments can often facilitate the safe navigation of a difficult experience. This approach acknowledges that challenging sessions can occasionally lead to significant therapeutic breakthroughs, making immediate chemical termination a secondary measure reserved for situations involving imminent risk of harm.
Conclusion
This review clarifies the pharmacological landscape for managing psychedelic-induced distress, identifying specific 5-HT2A antagonists and atypical antipsychotics as effective interventions. While several medications show promise, the current recommendations remain largely theoretically grounded and require rigorous clinical validation through human trials to establish standardized safety protocols. Future research must bridge this knowledge gap to ensure that pharmacological “trip killers” are used proportionally and safely within broader supportive care frameworks.