

Introduction
Headache disorders remain a leading cause of years lived with disability, often resulting in significant social and economic burdens. While the link between poor sleep and headache frequency is well documented, this study aimed to identify which specific sleep factors, such as hygiene, quality, or daytime sleepiness, serve as independent predictors of functional impairment. To ensure the integrity of the data, the research was conducted during interictal periods. This was defined as at least 48 hours following a migraine attack for EM patients or during a period of remission outside of an active cluster cycle for ECH patients. Crucially, none of the participants were receiving prophylactic headache treatments or psychiatric medications during the study. This exclusion of preventative therapy is vital as it ensures the observed sleep disturbances were not skewed by medications that commonly alter sleep architecture or autonomic function.
Infographic
Audio Summary
Key Findings
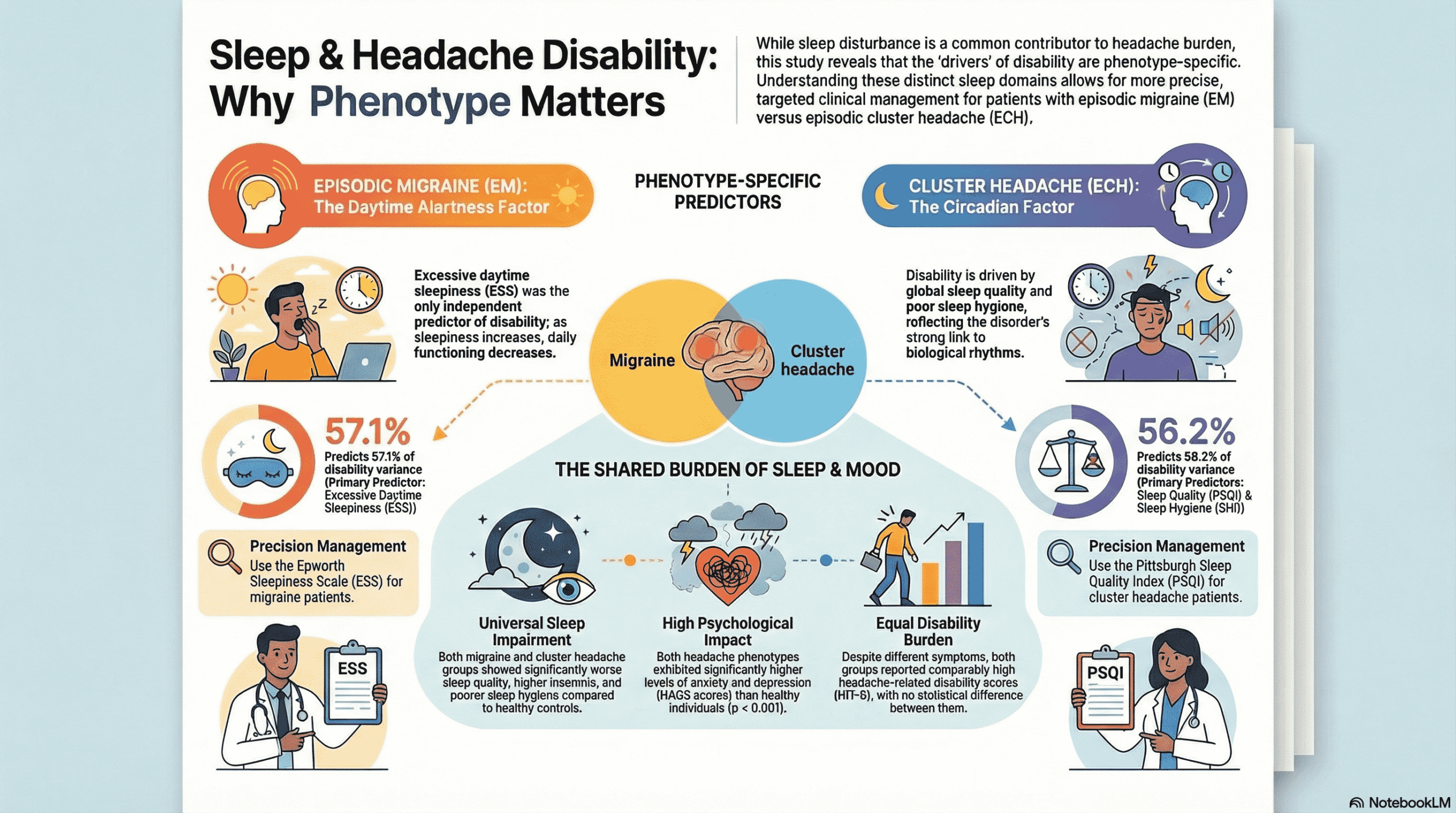
The study confirmed that patients with both episodic migraine and cluster headaches experience significantly higher rates of sleep disturbance, anxiety, and depression compared to healthy individuals. However, the researchers found that while anxiety and depression were prevalent, they did not independently predict how much the headache disorder interfered with daily life. This suggests that sleep issues impact functional ability directly, rather than simply acting as a byproduct of a patient’s mood.
For patients with episodic migraine, excessive daytime sleepiness was the only independent predictor of headache-related disability. Measured by the Epworth Sleepiness Scale, this suggests that the lack of alertness and drowsiness experienced during the day is the primary driver of impairment for migraineurs. Neurobiologically, this may be linked to how sleep fragmentation in migraine lowers the cortical excitability threshold, making the brain more susceptible to the activation of pain pathways.
In contrast, the predictors for cluster headache patients were global sleep quality and sleep hygiene. For this group, the consistency of sleep-related behaviors and overall restfulness were the factors most strongly associated with disability. This divergence is likely due to the intrinsically circadian nature of cluster headaches. Because these attacks are often locked to REM sleep and governed by hypothalamic dysfunction, poor sleep hygiene can further destabilize the body’s internal clock, exacerbating the functional burden of the disorder.
Conclusion
The results of this study underscore that treating sleep is not a one-size-fits-all solution for headache sufferers. The authors advocate for a phenotype-specific approach to clinical management, where interventions for migraine might prioritize daytime alertness while cluster headache strategies focus on stabilizing circadian rhythms through improved sleep hygiene. While these findings are exploratory and require replication in larger groups, they suggest that targeted sleep assessments can provide a more nuanced path toward reducing disability. Maintaining a sleep-focused perspective in clinical practice may offer a modifiable route to improving quality of life for those with these challenging neurological conditions.