

Introduction
Clinical practice frequently reveals an inverse correlation between serum vitamin D levels and the severity of hidradenitis suppurativa (HS), yet the causal direction of this relationship has remained a subject of debate. The purpose of this research was to utilize a dual methodology, combining a systematic review of existing literature with Mendelian randomization, to determine if low vitamin D is a primary cause of HS or merely a marker of the disease’s systemic inflammatory state. By incorporating Mendelian randomization, the researchers sought to overcome the limitations of observational studies, such as reverse causation and confounding factors, to provide a more objective assessment of the genetic drive behind the condition.
Infographic
Audio Summary
Key Findings
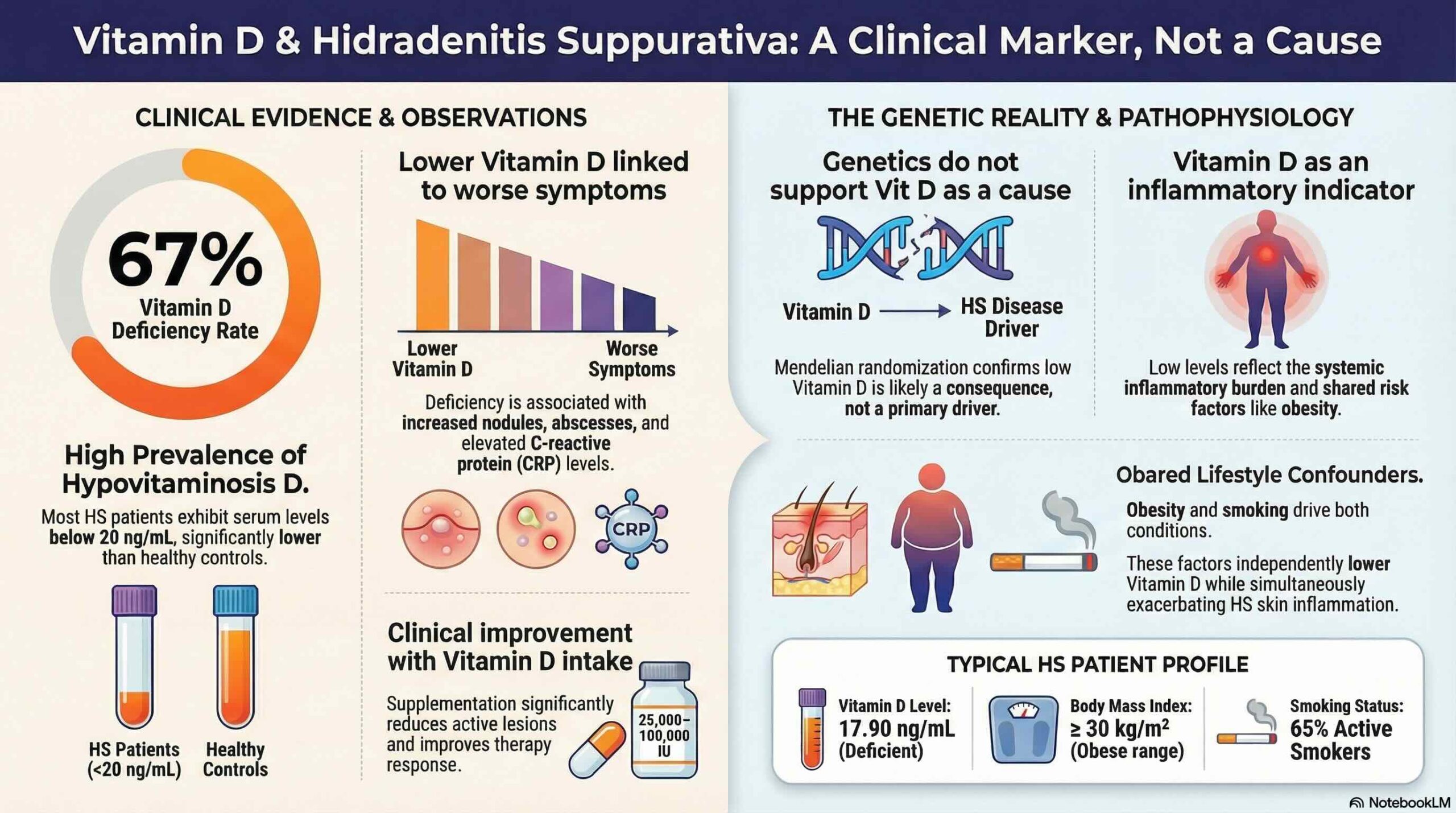
The systematic review synthesized data from 12 studies, confirming a significant prevalence of vitamin D deficiency among HS patients with a weighted mean of 17.90 ng/mL. The results demonstrated a consistent correlation between low serum levels and increased disease severity, the presence of active lesions, and elevated C-reactive protein (a common indicator of systemic inflammation).
To investigate causality, the researchers conducted a Mendelian randomization analysis using genetic data from the UK Biobank and FinnGen. This analysis produced a null estimate, which means it did not support a linear causal effect of lifelong, genetically predicted vitamin D levels on HS risk within the European-ancestry population studied. This suggests that while the two factors are linked in clinical observations, low vitamin D levels may not be the direct reason the disease develops.
Despite the lack of a direct genetic causal link, clinical supplementation has shown positive impacts on patient outcomes. Specifically, patients receiving vitamin D experienced clinical improvements such as a reduction in the number of active nodules and a lower frequency of flare-ups. This indicates that vitamin D may still function as a powerful modulator of the inflammatory environment, providing therapeutic benefits even if it is not the underlying cause of the disease.
Conclusion
Vitamin D deficiency in HS patients likely functions as a correlate of the systemic inflammatory state, lifestyle factors, or comorbidities rather than a primary cause of the disease. While vitamin D appears to have a modulatory role in inflammation, these genetic findings are specific to European-ancestry populations, and further interventional studies are needed to define its therapeutic application across diverse groups. Ultimately, vitamin D status should be viewed as an important marker of the broader inflammatory environment in HS rather than a standalone etiological driver.