

Background
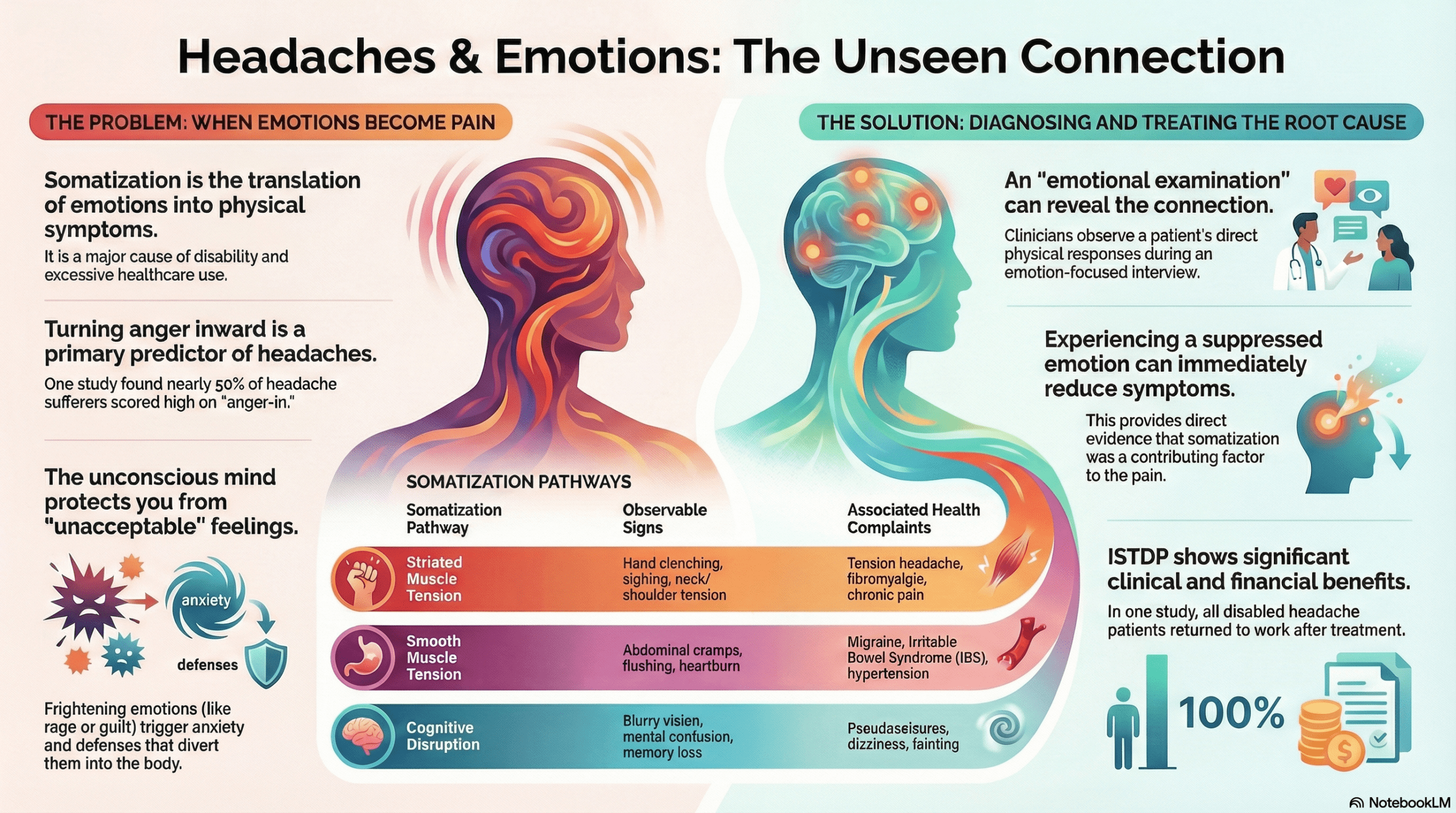
The research, conducted by Allan Abbass and Allan Purdy of Dalhousie University and David Lovas of Harvard Medical School, addresses the clinical phenomenon of somatization. In this context, somatization is defined as the translation of emotions into the development or exacerbation of physical symptoms.
This process imposes a massive burden on the healthcare system, accounting for a significant proportion of specialty medical visits, excessive diagnostic testing, and hospital utilization. Traditionally, these “medically unexplained symptoms” were diagnosed only after all organic causes were ruled out. The authors argue that this indirect approach is prone to diagnostic error and often denies patients access to targeted treatment for the underlying emotional drivers of their pain.
Infographic
Audio Summary
Navigating the Somatic Pathways of Emotion
The Problem of “Anger-In”
Clinical evidence highlights a robust correlation between chronic headache and difficulty regulating emotions—specifically anger. A key factor is “alexithymia,” a clinical construct describing an inability to identify or describe feelings. When a patient cannot name their distress, the psychological burden is forced into a somatic route.
Research indicates that the internalization of anger is a primary predictor of headache frequency and intensity. In experimental settings, migraine patients subjected to anger provocation exhibited significantly less overt anger behavior than healthy controls but experienced a significantly greater rise in pulse pressure. This objective physiological response underscores the “anger-in” phenomenon: while the emotion is suppressed behaviorally, it is discharged cardiovascularly. In study samples, nearly half of headache sufferers scored high on “anger-in” metrics, compared to only one-sixth of healthy controls.
Direct Diagnosis via ISTDP
To identify these drivers, the researchers utilize Intensive Short-Term Dynamic Psychotherapy (ISTDP). This methodology focuses on “observable physical responses” triggered during an emotion-focused interview, allowing clinicians to map the “Triangle of Conflict.”
The Triangle consists of three corners: Unconscious Feelings (the core emotion), Anxiety (the somatic discharge), and Defenses (the psychological mechanisms used to block the feeling). During the ISTDP assessment, the clinician monitors the patient for a shift from defense (e.g., intellectualization or smiling) to a breakthrough where the emotion is consciously experienced. When the patient experiences the feeling directly, the somatic discharge (anxiety) temporarily ceases, providing direct evidence of the link between emotion and pain.
The Four Somatic Pathways
The research identifies four distinct patterns of somatic discharge. Understanding these pathways allows clinicians to differentiate between tension-type headaches and vascular events like migraines.
|
Somatic Pathway |
Observations During Assessment |
Related Health Complaints |
|
Striated Muscle |
Hand clenching, sighing, neck/head tension, whole-body tension. |
Tension-type headache, fibromyalgia, backache, chest pain, fatigue. |
|
Smooth Muscle |
Absence of striated tension; abdominal cramps, heartburn, nausea, aura. |
Migraine, Irritable Bowel Symptoms (IBS), hypertension, bronchospasm. |
|
Cognitive-Perceptual Disruption |
Blurry vision, tunnel vision, mental confusion, loss of train of thought. |
Dizziness, fainting, pseudoseizures, memory loss, transient paranoia. |
|
Conversion |
Visible physical weakness or paralysis in voluntary muscles. |
Falling, aphonia (loss of voice), localized limb weakness. |
From Theory to Patient Care: A Case Study
The study details the psychodiagnostic evaluation of a 52-year-old woman suffering from 25 years of bitemporal headaches. Her condition had evolved from migraine without aura into Chronic Daily Headache (CDH). Despite clear neuroimaging and numerous medications, her “pounding” pain persisted.
During an ISTDP assessment, she exhibited classic striated muscle tension (clenched hands and sighing). When the interview mobilized feelings regarding her son’s defiance and her father’s emotional rejection, she uncovered repressed rage. As she consciously experienced this anger—described as an “urge to punch” followed by waves of guilt and grief—her muscle tension vanished. Crucially, her headache ceased during the session as emotional experience superseded somatization. A three-month follow-up showed significant sustained reductions in both pain intensity and frequency.
Clinical Outcomes
In a case series of 29 patients with unexplained headaches, the impact of addressing these emotional pathways was profound:
- Medication Reduction: Patients stopped 15 of 23 psychotropic medications, saving an average of $540 (CDN) per month in drug costs.
- Economic Impact: All seven patients previously disabled by their headaches returned to work. This resulted in a corporate savings of $16,400 (CDN) per month.
- System Efficiency: Treatment led to an 85% drop in hospital days over a three-year follow-up, with the cost of treatment being offset by healthcare savings within just four months.


Emotions can physically manifest as neurological tension when they are not consciously processed.
Authors Conclusions and Future Directions
The authors conclude that somatization is a prevalent, taxing factor in chronic headache care. They emphasize that the inability to experience complex feelings can directly exacerbate physical pathology. They recommend that physicians adopt emotion-focused interviewing and call for the development of a “standardized brief assessment interview tool” to screen for emotional factors. Furthermore, they advocate for formal Randomized Controlled Trials (RCTs) to validate ISTDP as a primary diagnostic and treatment tool for headache populations.
Conclusion
This research represents a vital shift toward a direct, observable diagnostic framework. By moving focus from ruling out organic disease to ruling in emotional discharge through the somatic pathways, clinicians can avoid the pitfalls of diagnosis by exclusion. This provides a clear, evidence-based pathway for patients who have otherwise exhausted traditional medical interventions.
However, clinical implementation requires nuanced consideration. The methodology necessitates specialized training and carries a risk of false positives or negatives if the clinician lacks focus or the patient is highly defended.
Ultimately, recognizing these pathways allows for more efficient medical investigations. When a clinician confirms an emotional driver for pain, they can bypass unnecessary, expensive testing and direct the patient toward life-changing psychological interventions. Understanding the “Triangle of Conflict” is not just a psychological exercise; it is a clinical necessity for improving long-term patient outcomes and reducing the systemic burden of chronic pain.
1 thought on “The Internalization of Anger as a Predictor of Chronic Headache”
This guys work is spot on. Excellent share.