


Introduction
The strategic necessity of this meta-analysis stems from a significant gap in the current neurosurgical literature. While stereotactic radiosurgery has been explored for nearly three decades as a treatment for cluster headache, reported outcomes remain inconsistent and the safety profile regarding deep neural structures is not fully established. Specifically, there has been a lack of clarity regarding how radiation affects the trigeminal nerve and the sphenopalatine ganglion (SPG) when targeted with submillimetric precision. The primary purpose of this study was to evaluate the pooled rates of pain relief, recurrence, and adverse radiation effects (AREs) across five major cohorts involving 51 patients.
Current first-line therapies for cluster headache include oxygen, triptans, and preventive medications such as verapamil. However, for patients who do not respond to these treatments, the search for non-destructive alternatives to historical ablative procedures, which often caused facial numbness and deafferentation pain, has led to the exploration of SRS. While the technical precision of SRS is exceptionally high, the clinical results synthesized in this review reveal a complex narrative regarding the durability of its effects.
Infographic
Audio Summary
Key Findings
The most critical takeaway from this research is the sharp dichotomy between early clinical success and long-term recurrence. For patients seeking permanent solutions, high initial success rates must be weighed against a significant decline in efficacy over time. This suggests that while SRS is effective at inducing an initial response, it likely acts as a temporary modifier of pain pathways rather than addressing the underlying central generator of the attacks, which is believed to be related to hypothalamic dysregulation.
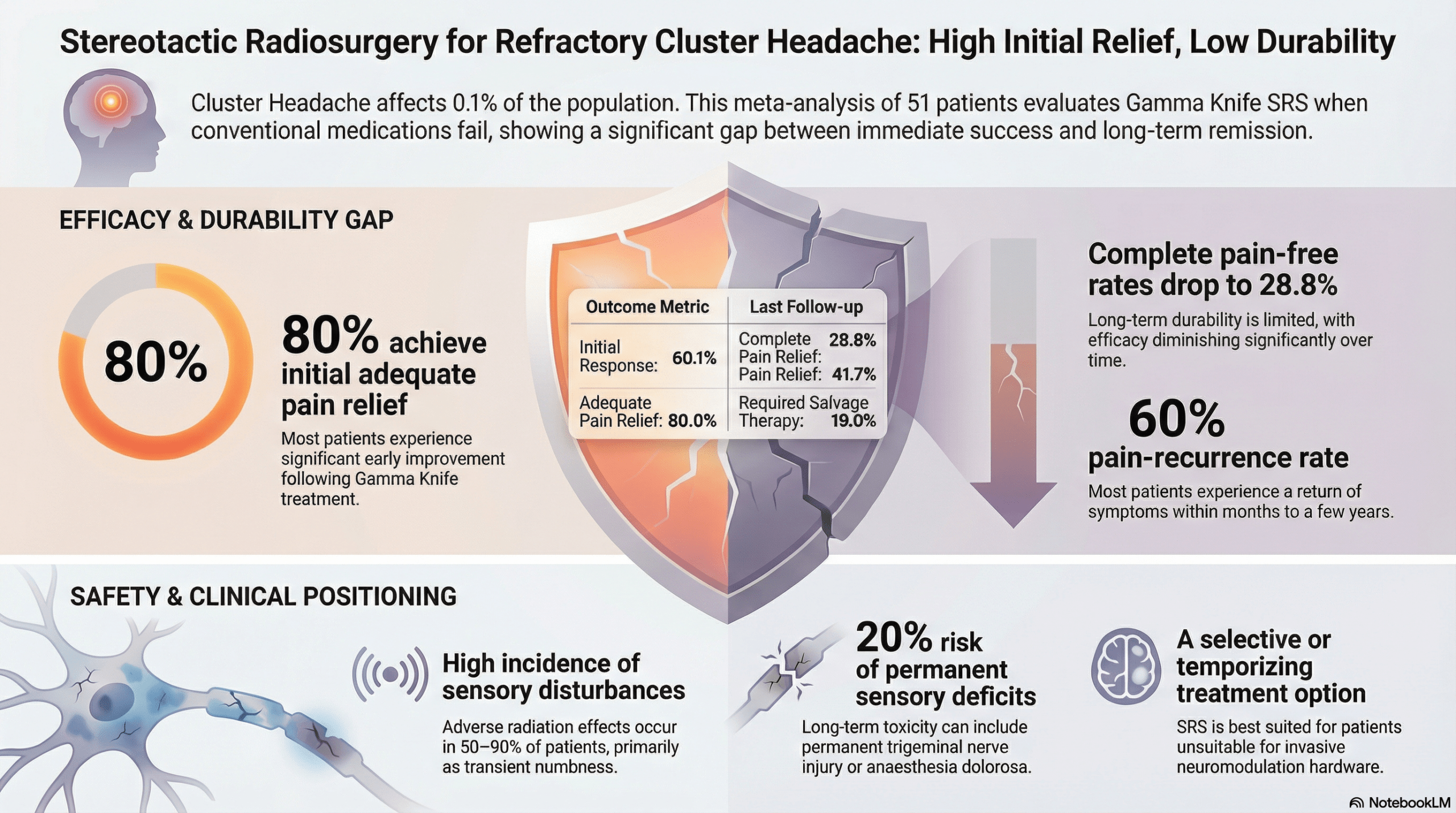
The data synthesis reveals the following primary outcomes:
Initial Efficacy: The study reported a 60.1 percent initial complete pain-free rate (95 percent CI: 24.4 to 91.3 percent) and an 80 percent initial adequate relief rate (95 percent CI: 67.0 to 91.0 percent).
Durability and Recurrence: These promising early figures stand in contrast to the results at the last follow-up before salvage therapy. Complete relief dropped to 28.8 percent, and the pain recurrence rate reached 59.8 percent.
Safety Profile: Adverse radiation effects were common, reported in 50 to 90 percent of patients. While many effects were transient, permanent trigeminal sensory deficits occurred in up to 20 percent of patients in certain cohorts.
The analytical depth of the study highlights that follow-up duration is a significant factor in reported efficacy, with meta-regression indicating that longer follow-up is significantly associated with lower pain-free rates (p = 0.011). Crucially, the meta-regression also identified patient subtype as a key moderator of success: the episodic subtype demonstrated greater sustained relief (p = 0.019) and a lower recurrence risk (p = 0.037) than the chronic subtype. Furthermore, a distinction in safety profiles emerged between historical and modern techniques. While earlier nerve-centered approaches were associated with high toxicity and severe complications like anesthesia dolorosa, more recent dual-target strategies involving the trigeminal nerve and SPG appear to offer a more favorable toxicity profile with lower rates of bothersome numbness.
Conclusion
The strategic placement of stereotactic radiosurgery in the cluster headache treatment algorithm should be as a temporizing or selective option. It does not currently serve as a direct competitor to deep brain stimulation (DBS), occipital nerve stimulation (ONS), or sphenopalatine ganglion (SPG) stimulation. DBS remains the only intervention with strong evidence for long-term remission in highly resistant cases, while ONS and SPG stimulation offer greater durability through reversible, non-destructive approaches. SRS is best utilized for patients who are unsuitable for or decline invasive device implantation.
The final assessment of this meta-analysis is a call for the cautious and highly selective use of SRS. While it offers a valuable non-invasive bridge to other therapies, its limited durability and the risk of permanent nerve injury require meticulous patient counseling. Future efforts must focus on multicenter prospective studies to optimize dual-target planning and standardize outcome metrics. This will ensure that the role of radiosurgery is clearly defined within the contemporary management of this debilitating disorder.