


Introduction
This systematic review holds significant strategic importance for the clinical community, particularly regarding the care of refractory patients who have exhausted conventional treatment avenues. Cluster headache is a primary headache disorder that predominantly affects men and is characterized by sudden, unilateral periorbital attacks lasting up to three hours. While initial management typically relies on high flow oxygen, triptans, and verapamil, a substantial percentage of patients remain non-responsive to these interventions. For these refractory individuals, the disorder remains a debilitating source of neurological morbidity. The purpose of this study was to measure the outcomes of various neuromodulation techniques, including vagus nerve stimulation (VNS), occipital nerve stimulation (ONS), deep brain stimulation (DBS), transcranial magnetic stimulation (TMS), and sphenopalatine ganglion (SPG) stimulation. By assessing metrics such as attack frequency, pain intensity, patient quality of life, and overall safety, the researchers sought to determine if these modalities offer a viable path forward. The investigators reached their conclusions by integrating data from multiple comprehensive databases, including PubMed, Cochrane, Web of Science, and Google Scholar.
Infographic
Audio Summary
Key Findings
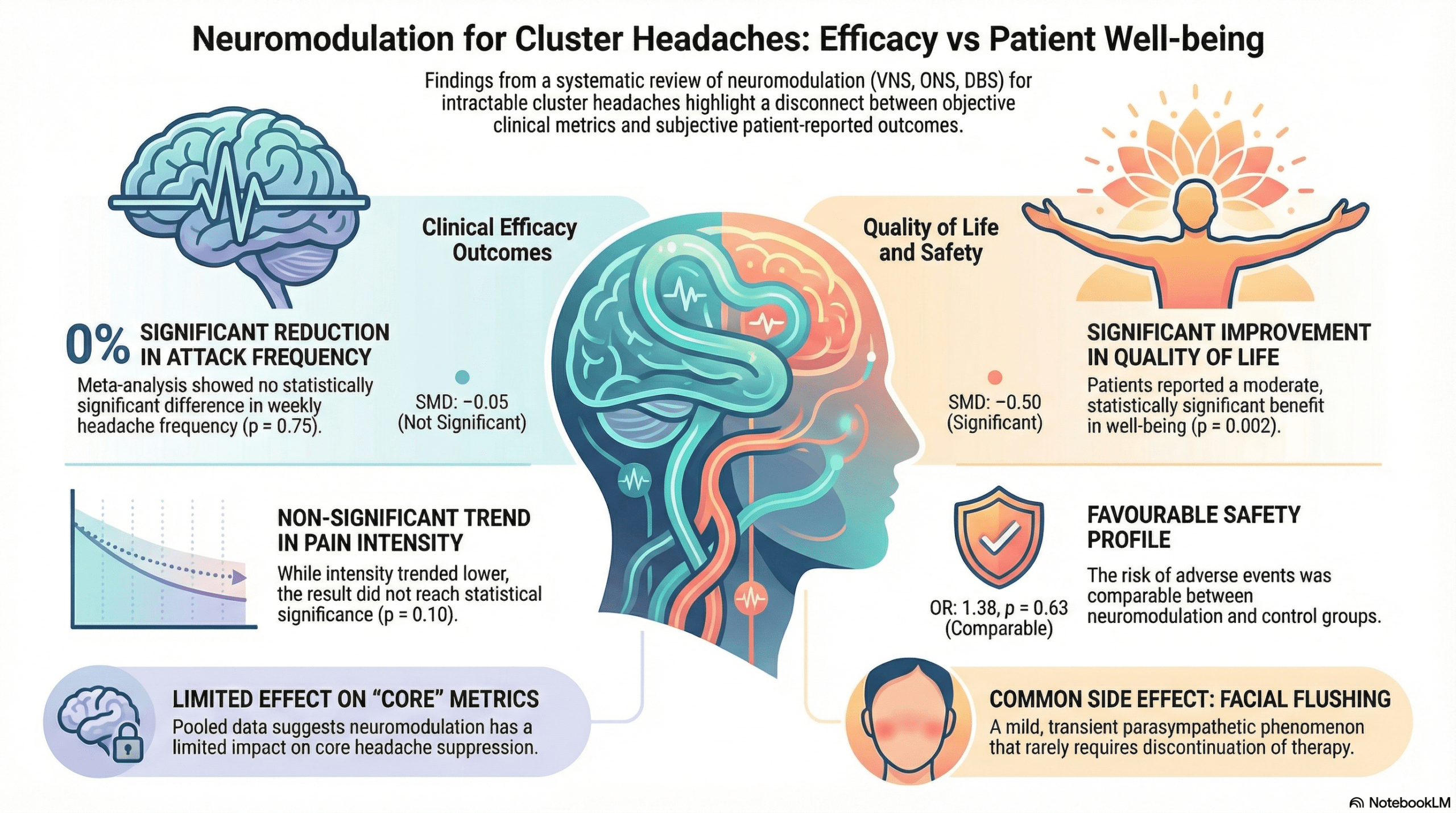
The findings of this meta-analysis offer a critical evaluation of the distinction between symptom suppression and overall patient well-being. When looking strictly at the primary efficacy outcomes, the data revealed no statistically significant difference in headache attack frequency or pain intensity between patients receiving neuromodulation and those in control groups. Specifically, the meta-analysis showed a standardized mean difference (SMD) for attack frequency of -0.05 (95% CI: -0.36 to 0.26, p = 0.75). Similarly, while pain intensity showed a slight downward trend, it did not meet the threshold for statistical significance with an SMD of -0.26 (95% CI: -0.57 to 0.05, p = 0.10).
The most compelling layer of this research, however, is the significant improvement in patient-reported quality of life. Despite the lack of measurable change in core headache metrics like the total number of attacks, neuromodulation demonstrated a significant positive impact on the daily lives of participants. The researchers reported an SMD of -0.50 (95% CI: -0.82 to -0.19, p = 0.002), which represents a moderate effect size favoring the intervention. This suggests that the success of a treatment may be felt by the patient even if it is not captured by traditional frequency counts. Regarding safety, the meta-analysis found that the overall risk of adverse events was comparable between the neuromodulation and control groups (OR: 1.38, 95% CI: 0.37 to 5.08, p = 0.63). A specific autonomic side effect, facial flushing, was noted to be higher in neuromodulation groups, yet it is characterized as a mild and transient parasympathetic phenomenon that typically does not necessitate the discontinuation of therapy. While these techniques appear generally well tolerated, the researchers noted high heterogeneity among the studies, which implies that results should be interpreted with caution. These mixed results highlight the broader challenge of defining success in chronic pain management, where improvements in well-being can occur independently of total symptom elimination.
Conclusion
Based on the scope of this systematic review, neuromodulation appears to be a safe and viable option for improving the quality of life for patients with refractory cluster headaches. While the evidence suggests these techniques do not serve as a definitive cure for the frequency or intensity of attacks, they provide a meaningful benefit to the patient’s overall experience of the disorder. These modalities should be considered on a case-by-case basis for those who have failed to find relief through standard pharmacological management.