

Introduction
There is a critical need to understand how the comorbidity profile and socioeconomic standing of individuals with cluster headache have evolved to better inform healthcare resource allocation. This research utilized Norwegian nationwide registry data from 2009 to 2022 to provide a comprehensive, hypothesis-free exploration of these trends. The strategic importance of this study lies in the mandatory and linked nature of the Norwegian registries, which utilize national identity numbers to ensure unified, nationwide coverage across primary and specialist healthcare. This robust dataset allows for a level of longitudinal detail and representativeness that previous smaller cohorts could not achieve, specifically regarding how health and social factors interact within a universal healthcare framework.
Infographic
Audio Summary
Key Findings
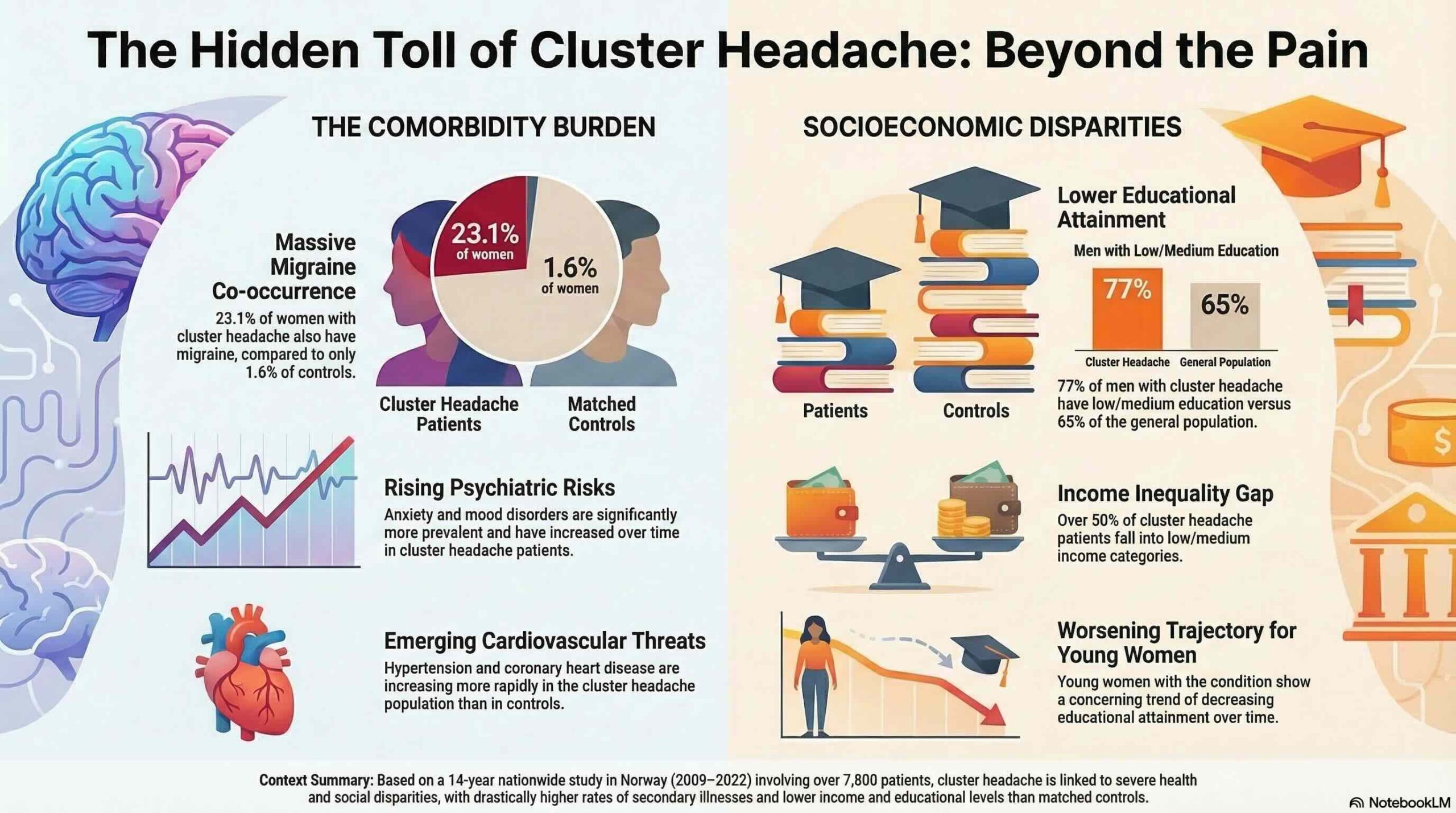
The analysis compared 7,803 people diagnosed with cluster headache against 387,042 matched controls. A substantial comorbidity gap was identified, most notably regarding migraine prevalence. Among women with cluster headache, 23.1% had comorbid migraine compared to 1.6% of controls, while 9.8% of men with the condition had migraine compared to 0.3% of controls. Individuals in the cluster headache group also exhibited significantly higher rates of mood disorders, anxiety, and cardiopulmonary issues, reflecting a high cumulative burden of illness.
Socioeconomic differentiators were equally pronounced. Low or medium income was recorded for 50.2% of men and 51.4% of women with cluster headache, contrasted with 42.2% and 46.6% in the respective control groups. Educational attainment followed this pattern of disadvantage, as 77.0% of men and 65.0% of women with the condition had low or medium levels of education, compared to 65.1% and 55.0% of controls.
The data highlighted concerning trajectories for specific demographics. Among women under 40 with cluster headache, the prevalence of low or medium educational attainment increased during the study period, while it decreased in the control group. Furthermore, hypertension in these young women showed an average yearly increase of 11.2%, a stark contrast to the 1% annual decrease observed in controls. Anxiety disorders in this same demographic rose by 11.3% each year, significantly outstripping the trends observed in the general population and underscoring the increasing vulnerability of younger patients.
Conclusion
These findings characterize cluster headache as a complex disease that requires specialized, individualized therapy and consistent clinical follow-up. The dual burden of health complications and socioeconomic disadvantages highlights the distinct vulnerability of this patient group. Clinicians and policymakers must recognize that effective management necessitates a comprehensive approach that addresses both the clinical comorbidities and the broader social implications of the condition to mitigate long-term disability.