


Introduction
Cluster headache (CH) is a primary headache disorder categorized as a trigeminal autonomic cephalalgia, characterized by excruciating, unilateral pain and debilitating autonomic symptoms. While standard pharmacological treatments exist, many patients remain treatment-resistant or develop significant intolerance to long-term preventive medications. This necessitates the development of effective interventional options like peripheral nerve blocks to bridge the gap in care. The primary objective of this study was to determine if a combined approach targeting multiple pathways provides a clinical advantage over the standard, single-point greater occipital nerve (GON) block. This comparison is vital for evolving the current treatment algorithms for refractory cluster headache cases.
Infographic
Audio Summary
Key Findings
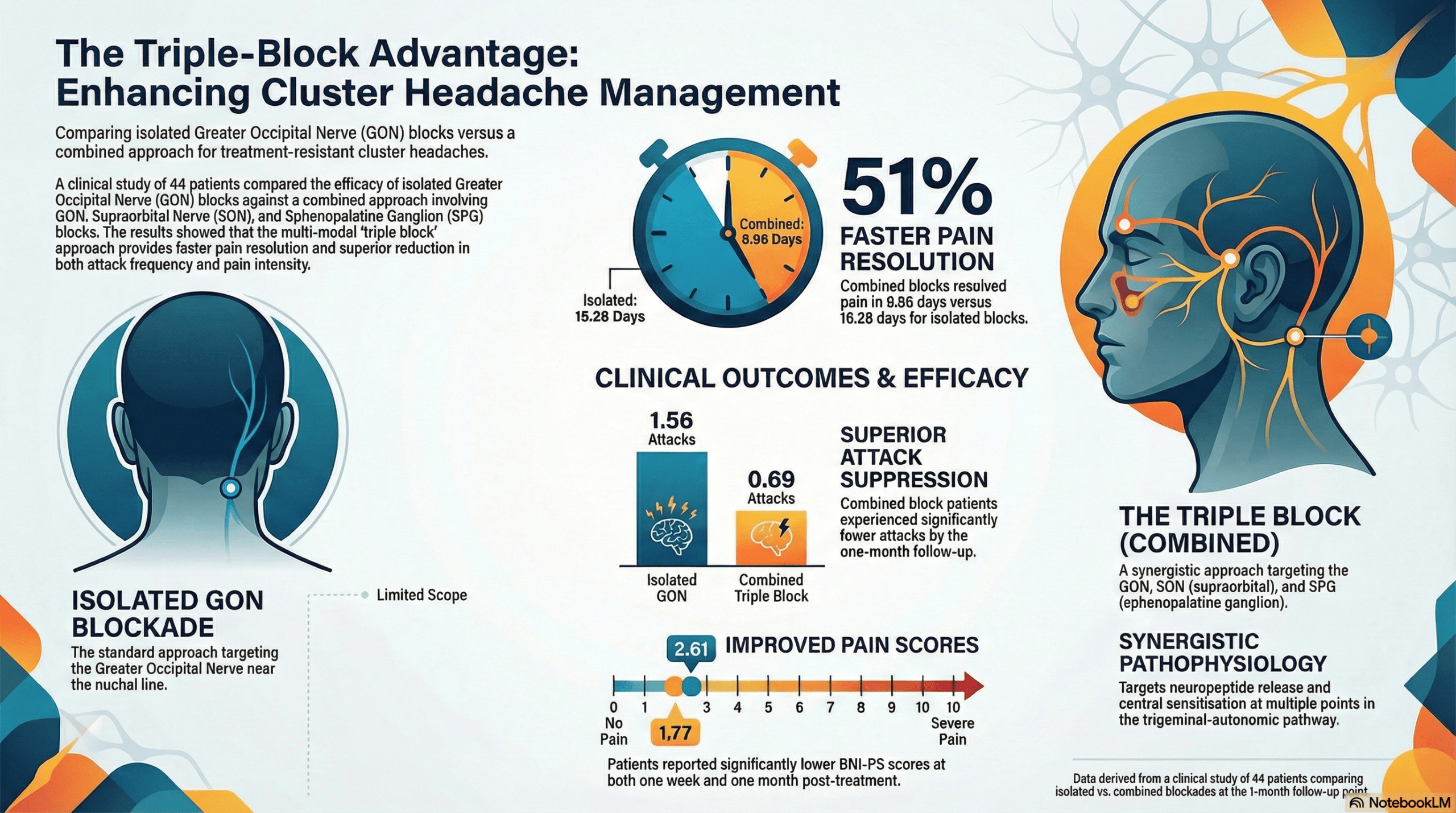
The retrospective analysis followed 44 patients at Ankara Bilkent City Hospital, comparing 18 individuals who received an isolated GON block to 26 who received a combined intervention of GON, supraorbital nerve (SON), and sphenopalatine ganglion (SPG) blocks. While both groups benefited from the interventions, the combined blockade group demonstrated significantly superior outcomes across all clinical metrics, including a more robust reduction in attack frequency at both one-week and one-month intervals.
The clinical significance of these findings is most evident in the pain intensity scores. Patients in the combined group achieved a mean Barrow Neurological Institute Pain Scale (BNI-PS) score of 1.77 at the one-month mark, indicating a transition toward a state of no pain or only occasional pain. In contrast, the GON-only group maintained a higher mean score of 2.61, leaving many patients in the category of mild pain that still requires medication for control. Furthermore, the combined approach proved to be twice as efficient, with the duration until pain resolution averaging approximately 9 days compared to 18 days in the isolated GON group.
The superior efficacy of the triple-blockade strategy is likely due to the simultaneous inhibition of the trigeminal-autonomic reflex at multiple points. From a biochemical perspective, GON blockade reduces levels of calcitonin gene-related peptide (CGRP) and substance P, while SPG blockade inhibits the release of nitric oxide and vasoactive intestinal peptide (VIP). By adding SON blockade to interrupt nociceptive inputs and reduce cortical pain perception, this multi-modal strategy modulates the hypothalamic-trigeminal-autonomic pathway more effectively than single-point interventions.
Conclusion
This study provides compelling evidence that combining GON, SON, and SPG nerve blocks represents a necessary evolution in the management of cluster headache. The results suggest a paradigm shift from isolated nerve blocks to multi-point interventional strategies, particularly for treatment-resistant patients who require rapid and potent relief. By targeting various neuropeptides and central sensitization mechanisms simultaneously, clinicians can achieve faster pain resolution and a significantly lower attack burden than previously possible with standard methods.