

Introduction
The establishment of the Korean Cluster Headache Registry (KCHR) serves as a vital strategic instrument for correcting the widespread myth that this condition is a rare curiosity in the region. By coordinating data across 16 tertiary hospitals, the initiative seeks to dismantle the diagnostic delays and systemic undertreatment that have historically stemmed from insufficient data. This transition from sparse historical anecdotes to a rigorous, prospective framework allows for a more accurate characterization of the disease burden in Korea. As systematic data collection replaces outdated assumptions, the registry provides the evidence needed to modernize local clinical practices and align them with international neurological standards.
Infographic
Audio Summary
Key Findings
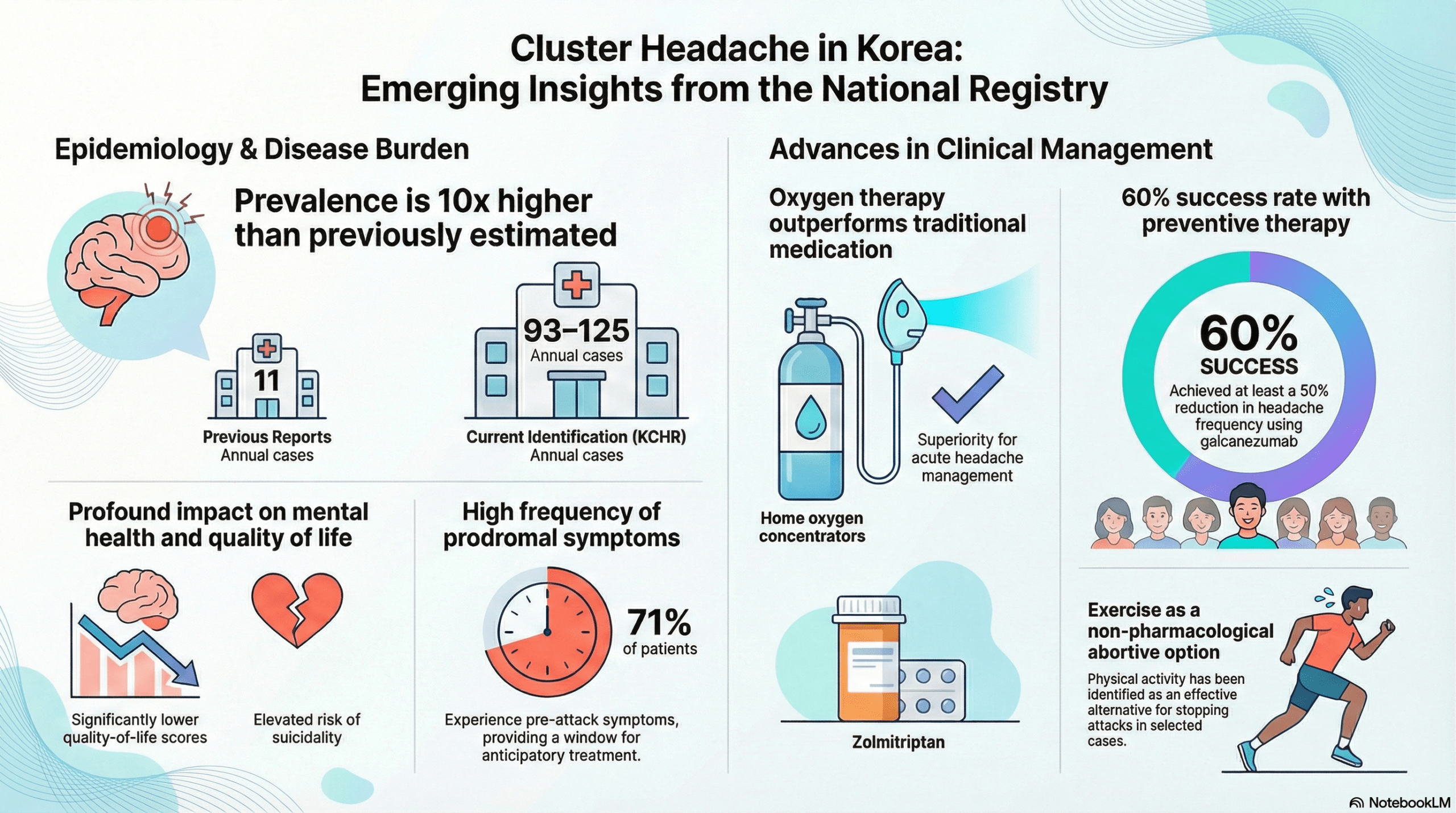
The registry data effectively redefine the epidemiological scale of the disorder, identifying 93 to 125 annual cases across the participating centers. This volume significantly exceeds previous estimates that suggested as few as 11 cases per year. While male predominance remains clear, the study identifies a distinct bimodal onset in women, with peaks occurring during the second to third and fifth to sixth decades of life. Women also exhibit higher rates of comorbid migraine and chronic cluster headaches. Smoking was identified as a specific aggravating factor closely linked to the development and severity of the chronic subtype.
The psychosocial impact of the condition is substantial. Patient quality of life, measured by EQ-5D scores, was significantly lower at 0.88 compared to 0.99 in healthy control groups. There is also a documented increase in suicidality risk among those affected, highlighting the severity of the pain experience. Clinical warning signs are remarkably common, as 71 percent of patients reported pre-attack symptoms and 35 percent identified pre-cluster symptoms. These prodromal markers offer a potential window for early intervention and improved patient preparedness before the full onset of a cluster bout.
Management strategies have also been modernized through KCHR insights. Oxygen therapy delivered via home concentrators proved superior to zolmitriptan for acute relief, offering better patient reported outcomes. Additionally, exercise emerged as a unique patient driven alternative for aborting attacks in specific cases. For prevention, the CGRP monoclonal antibody galcanezumab demonstrated high efficacy, with more than 60 percent of patients achieving at least a 50 percent reduction in attack frequency. These findings fundamentally restructure the clinical landscape for Korean patients by emphasizing multi modal and personalized care strategies.
Conclusion
The findings from the KCHR necessitate a comprehensive revision of regional diagnostic and therapeutic guidelines to ensure they reflect the actual prevalence of cluster headaches. Early recognition of prodromal features and the prompt application of modern therapies such as CGRP monoclonal antibodies are essential for reducing the long term psychosocial burden of the disease. By aligning Korean data with broader Asian epidemiological trends, this study underscores that the condition is not rare but rather historically underdiagnosed. This work provides a definitive foundation for improving clinician awareness and elevating the standard of headache medicine across the continent.